
This post was co-authored with Rachel Hardy, M.A.
In this three-part post, we seek to explore alternate explanations for childhood defiance/misbehavior. In Part 1, childhood misbehavior was conceptualized as potentially normative and may even be indicative of healthy psychological development. Here, in Part 2, childhood misbehavior is considered as a potential symptom of an otherwise difficult-to-notice mental health problem.
As stated in Part 1, parents and clinicians alike may be tempted to label children who exhibit repeated acts of defiance or misbehavior as “oppositional/defiant.” Oppositional defiant disorder (ODD), with an estimated adolescent prevalence of up to 12.6% [8], is a diagnosis that encompasses many behavioral symptoms relating to misbehavior, angry/irritable mood, argumentativeness/defiance, and vindictiveness. This means that children who meet the criteria for ODD often lose their temper, get annoyed easily, argue, defy requests/rules, and act in a spiteful, aggressive manner towards others. In short, children labeled with ODD are often seen as inherently oppositional and temperamentally difficult or vindictive.
However, making these types of characterological attributions could do more harm than good—they don’t produce any workable solutions and may even distract from a real underlying psychological problem. In fact, ODD itself is likely best understood as a label for a cluster of behavioral symptoms rather than an underlying cause of those behavioral symptoms. While this post has no intention to delve into the moral implications of childhood misbehavior, it's worthwhile to explore other clinical explanations of childhood defiance that may help parents address the real root of the problem.
This post uses clinical and research evidence to suggest three possible causes for childhood misbehavior in an effort to defend the character of the so-called "defiant child" and help parents stay aware that acting out can be a symptom of an underlying clinically significant problem that might otherwise go unnoticed.
1. Defiance may be a sign of anxious distress
In the last post, general emotional distress (e.g., anxiety, sadness) was mentioned as a potential root cause of defiance and misbehavior. Below, we take a more nuanced approach and discuss the link between disruptive behavior and disorders of anxiety specifically. About 40% of children who meet the criteria for ODD also meet the criteria for an anxiety disorder [11]. This means that almost half of all children who exhibit clinically significant behavior problems also experience a clinically significant amount of anxiety. That's an astonishing comorbidity rate. Researchers have sought to untangle the direction of effects regarding the two types of disorders, and like many things in life, it's a complicated matter that depends on the myriad individual and environmental factors. However, what is clear is that at times, oppositional and defiant behavior can be rooted in intense feelings of anxiety.
Children with anxiety disorders exhibit excessive worries, fears, and anxiety that may be general and span different domains of life (as with generalized anxiety disorder) or specific to a particular type of situation (as with social anxiety or separation anxiety disorder). One of the key features of all anxiety disorders is that the person finds it difficult to control his or her worrying. This means that when children suffer from untreated anxiety disorders, they may have an exceptionally hard time coping or regulating their emotions when placed in anxiety-inducing situations—at times becoming defiant or oppositional as a result. In Part 1, we discussed childhood defiance as a form of control-seeking in uncertain, anxiety-provoking situations or a form of (faulty or misleading) self-expression when unable to articulate an intense emotional experience in a more socially acceptable way. Both explanations remain likely scenarios for children with anxiety disorders.
Additionally, when fear and anxiety are more acute, children may become oppositional simply in an effort to escape the situation that makes them feel such emotional distress. This is called “avoidance,” and children and adults alike go to great lengths to steer clear of the things that they fear the most in life. For example, a child that meets the criteria for separation anxiety disorder may exhibit persistent reluctance, and even downright refusal, to go to school because of an intense fear about leaving loved ones. While this behavior could easily be construed as opposition and defiance, a further assessment of the child’s internal states would reveal the true cause of the disruptive behavior.
2. Defiance may be a sign of depression symptoms
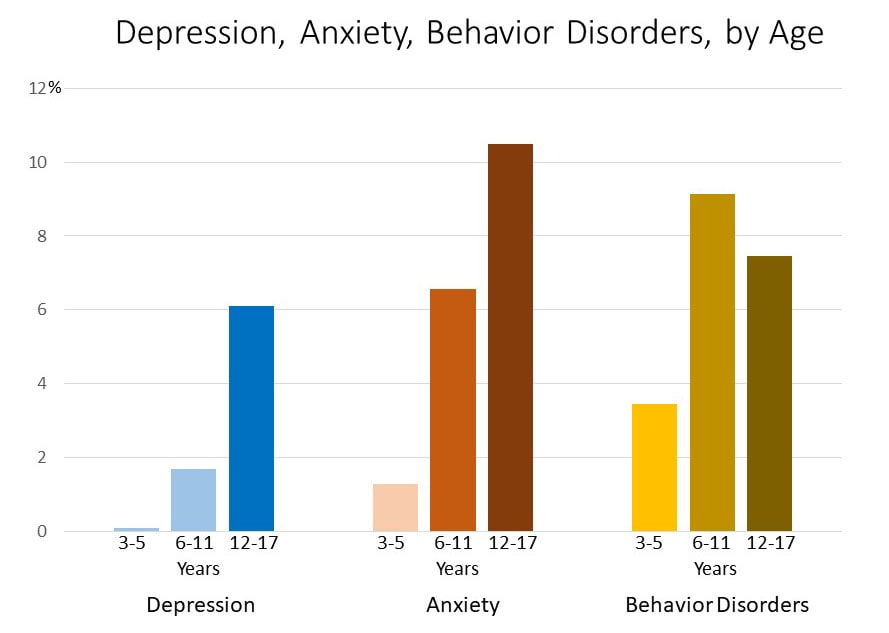
Based on data collected from nationally representative samples [2,7], the Centers for Disease Control and Prevention has put together information about the prevalence of depression, anxiety, and behavior problems in children across three age groups (see here and below).

Of these three types of disorders, depression is the least common, however, among older children, depression has an occurrence rate of greater than 1 in 20. And, although this prevalence rate is fairly low, individuals can have symptoms of depression without exceeding the threshold necessary for a diagnosis of depression. With this in mind, it's worth considering the possibility that older childhood misbehavior may be a sign of depression symptoms.


Especially given that irritability is a key diagnostic feature of depression in children and adolescents [1], one can quickly make the logical jump to understand that a depressed child might be predisposed towards acting out. Imagine if 14-year-old Jess, who lives a fairly average daily life, experiences none of the normative daily highs that her peers do. She doesn't enjoy her elective art class, she doesn't feel excited when her team wins in gym class, and she doesn't grow eager to get home at the end of the day. Instead, her mood exists somewhere between flat emptiness and mild grumpiness. How much more likely is Jess to react unpleasantly in response to her parent's request to take out the trash than her peers might be? For the adolescent who experiences more-than-average symptoms of depression (regardless of qualifying for clinical diagnosis), simple inconveniences and tasks are not buffered by the daily highs experienced by most children. As a result, Jess may react to her parent in a defiant manner—or even break down into tears of frustration. Signs like this suggest that the child may be experiencing some emotional turmoil rather than that they are a defiant child.
3. Defiance may be a symptom of traumatic stress
Finally, childhood defiance may be rooted in previous exposure to a traumatic event. The way children react to trauma can often look a lot like oppositional defiance, and indeed, a large percentage of children who are exposed to trauma subsequently exhibit dramatic changes in behavior that map quite well onto the symptoms described by ODD [6].
Childhood traumatic experiences take many forms—exposure to violence, medical trauma, and natural disasters, to name a general few. These are events that pose serious emotional or physical injury or even threaten death to the child [1,5]. To be clear, these events threaten a child’s sense of physical or emotional safety in a way that major life stressors (e.g., parental separation/divorce, parental remarriage, moving) do not [3]. Most children who are exposed to traumatic events experience initial high levels of distress that diminish over time—it is well established that most individuals naturally recover from traumatic stress [9]. However, there is a subset of children who do continue to experience long-term effects of trauma, such as behavioral problems, poor emotion regulation, physical health problems, and academic struggles [4]. Indeed, like many things in life, reactions to trauma exist on a spectrum—child reactions to trauma vary widely, and at times, defiance, temper loss, and other disruptive or destructive behaviors may occur [9].
So how exactly can trauma lead to childhood defiance? To quote researchers Perry and Pollard [10], “All experiences change the brain, but not all experiences affect the brain equally” (p. 33). Traumatic events are uniquely threatening and may cause impairments in the function of several brain areas responsible for emotional and behavioral regulation (more detail on how trauma affects the brain). These impaired neurophysiological processes often render a child more likely to be reactive to everyday stressors, leaving him or her feeling unsettled and leading to emotional and behavioral outbursts [10]. In other words, children whose brains have been deeply affected by a traumatic event are more likely to “overreact” or become defiant, especially in situations that threaten the child’s sense of safety or well-being.
Take, for example, an all-too-common form of childhood trauma: repeated and incessant bullying. Imagine Johnny, who is in third grade, goes to school every day where his peers laugh at his clothes, push him into the walls when the teacher isn’t looking, and even spit on him. Like many children who are survivors of bullying, he feels powerless and defenseless while this is happening. Soon, Johnny starts to hate going to school. Even the thought of going to school triggers a physical reaction—blood rushes to his face, his stomach gets all knotted up, he loses his appetite. He starts to refuse to get on the bus in the morning, throwing tantrums or running away from his parents. He might even refuse to do his homework in the evenings because it reminds him of his experiences that day at school. Surely, these acts of outward defiance are not rooted in an oppositional temperament or a flaw in his parents’ parenting skills—they are an entirely reasonable reaction to an extreme situation in which Johnny’s very well-being is threatened!

Why is labeling accurately—or, just as importantly, choosing not to label—so meaningful? The defiant label stigmatizes the child as inherently “bad” or comparatively worse than other children. This has implications relating to self-esteem, self-fulfilling prophecy, and parental interventions. Additionally, viewing defiance as a fundamental personality flaw could lead to two equally dangerous outcomes: it could absolve parents and child of the responsibility to be agents of change, since personality is often viewed as relatively stable, or it could lead to parents feeling hopeless about ever-improving their child’s behavior and perhaps even giving up trying. It should be noted that our hope is not to discourage parents from seeking treatment for their child's misbehavior, but rather to empower parents with knowledge about defiant behavior so that they are better equipped to tackle their child's behavior problems.
See Part 1 of The "Defiant" Child here, and continue reading Part 3 here.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-V (5th ed). Washington, D.C: American Psychiatric Association.
Bitsko, R. H., Holbrook, J. R., Ghandour, R. M., Blumberg, S. J., Visser, S. N., Perou, R., & Walkup, J. T. (2018). Epidemiology and impact of health care provider-diagnosed anxiety and depression among US children. United States.
Dubow, E. F., & Rubinlicht, M. (2011). Coping. In B. Brown & M. Prinstein (Eds.), Encyclopedia of adolescence (pp. 109–118). San Diego, CA: Academic Press.
Felitti, V., Anda, R. F., Nordenberg, D. F., Williamson, D. F., Spitz, A. M., Edwards, V., … Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine, 14, 245–258.
Finkelhor, D., Turner, H. A., Shattuck, A., & Hamby, S. L. (2015). Prevalence of childhood exposure to violence, crime, and abuse: Results from the National Survey of Children’s Exposure to Violence. JAMA Pediatrics, 169, 746–754.
Ford, J. D. (2002). Traumatic victimization in childhood and persistent problems with oppositional-defiance. Journal of Aggression, Maltreatment & Trauma, 6(1), 25-58.
Ghandour, R. M., Sherman, L. J., Vladutiu, C. J., Ali, M. M., Lynch, S. E., Bitsko, R. H., & Blumberg, S. J. (2019). Prevalence and treatment of depression, anxiety, and conduct problems in US children. United States: Elsevier Inc. doi:10.1016/j.jpeds.2018.09.021
Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry. 2010;49(10):980–989
National Institute of Mental Health. (May 2019). Post-Traumatic Stress Disorder. Retrieved from https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-p…
Perry, B. D., & Pollard, R. (1998). Homeostasis, stress, trauma, and adaptation: A neurodevelopmental view of childhood trauma. Stress in Children, 7(1), 33–51.
Drabick, D. A. G., Ollendick, T. H., & Bubier, J. L. (2010). Co-occurrence of ODD and Anxiety: Shared risk processes and evidence for a dual-pathway model. Clinical Psychology, 17(4), 307-318.


{kind=link}