
Cognitive Behavioral Therapy
CBT Versus Psychodynamic? No!
It is wrongheaded to define CBT against PD as if they were horses in a race.
Posted January 10, 2014
A quick glance across the field of psychotherapy reveals a fragmented mass of approaches. Yet despite the general chaos, it is also the case that there are two broad streams of thought, cognitive behavioral (CBT) and modern psychodynamic (PD), which continue to compete for overall dominance. Many practitioners describe their orientation as one or the other, many programs in professional psychology teach primarily one or the other, and there have been many research trials comparing one to the other in terms of overall outcomes (see here, here, and here for examples). CBTers are more dominant in the university settings because they tend to be more tied to conducting research, and, consequently, nowadays most in professional psychology are initially trained in CBT. However, at least relative to the university setting, PD is more prominent in the world of practice. It is also the case that many programs and practitioners are “eclectic” in that there are a growing number that see the two approaches as each having value and they borrow from both.
Unfortunately, all of this is an asinine way of thinking about these issues and is bad for the future of psychotherapy. Why? Because the essence of CBT, boiled down to its core, is a set of technologies that foster training skills to reduce problematic psychological symptoms. PD, at its core, is about gaining insight into one’s identity and relationship patterns in a way that fosters deeper awareness and more adaptive living. So, now ask yourself: Is it better for psychotherapy to focus on strategies that reduce problematic symptoms or is it better to focus on gaining deeper insight into one’s identity and relationship patterns? You don’t need a doctorate in professional psychology to know that this is an idiotic way of framing the issues. Yet, that is essentially what our field does. Our fragmented ideologies are so deeply entrenched that it is hard to see how bass ackwards they are.
Let me be very clear. A proper understanding of both the science of human psychology and the research in psychotherapy makes it obvious that the “CBT versus PD” framing of training, approaches, outcomes, etc. is completely wrongheaded.
Why do we have such a misguided division, entrenched in the training and practice of psychotherapy? Because the philosophical and theoretical frameworks and communities that CBT and PD historically emerged from are distinct, and both carry important truths and significant errors. As such, both have value and both are limited. In addition, the strengths in one approach tend to parallel the weaknesses in the other, and vice versa. Thus, not unlike political parties, these paradigms have grown as competing ideologies that became defined against one another in the battle for prestige, power and legitimacy. And now the most enlightened say that both have strengths and we can draw on both. Yet even this approach is problematic because it implicitly legitimizes the root problem. It isn’t that we should “teach them both.” Instead, we should have an understanding of human psychology that allows us to see how silly it was that they have been defined against one another for so long in the first place.
What is the right way to go?
First, we need to teach students an integrative meta-theoretical framework that allows them to assimilate and integrate the findings from human psychology into a coherent way. (See here for such an approach).
Second, we need to recognize psychotherapy as a formal relationship established with a professional trained in the values, knowledge base, and skills in applying the science of human psychology with the purpose of assisting the individual toward what the participants deem to be more valued and adaptive ways of being.
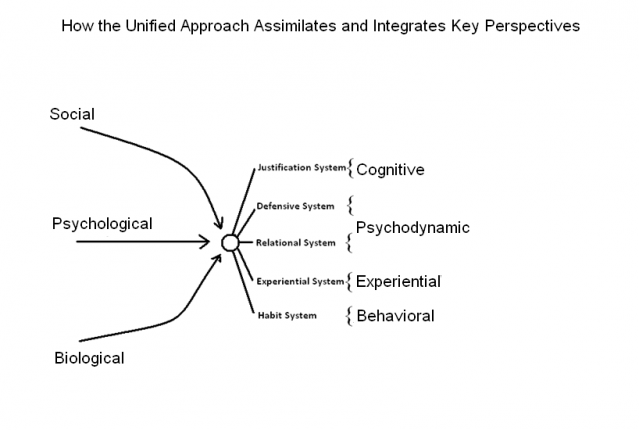
Third, we need to see individual psychotherapy as fostering character adaptation, in various ways and levels of depth. Your character is your idenity and the process by which you interact with your environment (you also have temperamental and ability dispositions as part of your personality). There are five systems of character adaptation: 1) the habit system; 2) the experiential system; 3) the relationship system; 4) the defensive system; and 5) the justification system. (See here for details on each system and here for applying them in psychotherapy).
Via this lens, one can see in a straight forward way that the major systems of psychotherapy line up with the systems of adaptation. Specifically, the behavioral tradition corresponds to the habit system, the experiential and emotion focused traditions correspond to the experiential system, the psychodynamic tradition corresponds to the relational and defensive systems, and the justification system corresponds to the cognitive and existential traditions.
Understood this way, one sees that the two dominant models of psychotherapy as emphasizing different systems of character adaptation. CBT tends to emphasize change via the habit and justification systems (i.e., actions and beliefs). In contrast, modern PD practitioners tend to emphasize the experiential, relational, and defensive systems of adaptation (i.e., core feelings, primary relationship schema, and subconscious processes). From a unified psychotherapy perspective, although there are times in which it might be appropriate to focus more on one system relative to the other, each person and each problem is made up of all these systems of adaptation operating in a socio-historical-organic context and practitioners should be able to assess and treat all of these systems.
Let’s conclude this argument with an imaginary parallel from medicine. Imagine if the field of medicine was divided into two large camps of medical doctors. Some MDs, let’s call them “GIRs,” believed that the key to physical health was the understanding of and treatment of the gastro-intestinal tracts and reproductive systems. As such, they emphasized the crucial importance of food and sex and reproductive health. In contrast, other MDs were “MCs”, who believed that the key treatments should focus on the muscular-skeletal and circulatory systems. They emphasized the importance of exercise, body form, and fitness. Whole programs, training models, and practitioners, and research trials all competed about these two visions of physical health. The emerging, enlightened consensus is—surprise, surprise—suggestive that both perspectives have validity...
I’ll end this post with one of my favorite quotes from Jeffrey Magnavita, who is a pioneer in advocating for unified approaches to the field of psychotherapy…
Psychotherapists behave like members of competing tribes, with different esoteric languages and rituals. Unification assumes that we all work in the same realm with the same processes regardless of the subsystem or specific domain we emphasize and specialize in. A unified model encourages us all to be aware of the larger picture and even if domain-specific treatment is undertaken, an understanding of the system and interconnections of domains and processes keep us alert to other possibilities for further developments.

