
Asperger's Syndrome
Hysteria: A Historic Anti-Asperger-Syndrome Syndrome?
Hyper-mentalism explains the puzzling, protean symptoms of hysteria.
Posted March 6, 2014
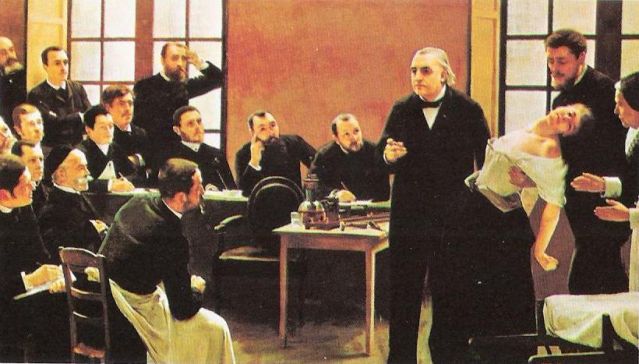
What sense can anyone make of hysteria? The great Jean-Martin Charcot (1825-93) made his reputation with it — at least during his reign as the Napoleon of the Neuroses at the Salpêtrière, which he turned into the world’s leading hospital for hysterics. But as Asti Hustvedt recounts in her study of hysteria in 19th-century Paris, following his sudden death, the show was over. Charcot's leading ladies (for nearly all hysterics were female) lost their careers as heroines of hysteria (often along with some of their symptoms), and disciples such as Tourette (looking on at the front above) or Babinski (supporting Blanche, the prima donna patient) lost not simply their leader, but their faith in his doctrine of the disorder. Freud had attended the Tuesday lectures illustrated here along with much of Parisian intellectual society, and of course went on to make a name for himself as a student and a (self-proclaimed) success as a therapist of hysteria.
But today the disease is extinct, and newer ones have taken its place: such as Multiple Personality Disorder (MPD). Once extremely rare, MPD grew to quasi-epidemic proportions in Anglo-Saxon countries and Holland after the 1970s, but without affecting other countries, somewhat as hysteria did. Nevertheless, MPD — or at least, dual personality — was a symptom seen in some hysterics, and indeed became the centerpiece of Jules (younger brother of Pierre) Janet’s theory of hysteria. And the varied symptoms of hysteria could be reproduced in hypnosis to such an extent that other influential theories of the disorder linked the two explicitly. Furthermore, many symptoms, whether induced by hypnosis or part of the hysteria such as anesthesia, were genuine: no hysteric could pretend indifference to having a needle pushed right through a hand or arm unless the limb was indeed anesthetic!
So what do we really know about hysteria? Most authorities would probably agree on the following points:
- Hysteria was a historically- and culturally-contingent diagnosis, which has failed the test of time unlike some of Charcot’s other discoveries, such as amyotrophic lateral sclerosis (alias Lou Gehrig’s disease in the USA, Charcot’s disease in Europe).
- Although also occasionally diagnosed in men, hysteria mainly affected women.
- The disorder shared many features with hypnosis, which could reproduce or remove signs and symptoms, but not cure them permanently.
- Such was the suggestibility of hysterics that hysteria often had elements of Folie à deux/shared psychotic disorder (DSM IV) to the extent that the hysteric’s symptoms and responses were closely tied up with her doctor’s expectations and beliefs about the illness.
- Hysterics were widely suspected of deceit, with physicians commenting that “One common characteristic unifies hysterics: instinctual simulation, an inveterate and incessant need to lie for no reason and no end, simply in order to lie.”
- Hysterics sometimes produced symptoms otherwise seen in religious manias or demonic possession, such as hallucinations or stigmata (cutaneous symptoms, most astonishingly, dermagraphism: words or images which could literally be written on the skin, and could persist for days or weeks).
- Some gifted hysterics could portray emotion with such dramatic skill that famous actors — notably Sarah Bernhardt — studied with them and imitated them in their performances.
- Writers, novelists, and artists were fascinated by hysteria, and doctors — significantly, but not exceptionally, Freud — explicitly recognized parallels between the case histories of hysterics and works of fiction. Indeed, the surrealist, André Breton, called hysteria “the greatest poetic discovery of the late 19th century.”
- Finally, some signs and symptoms of hysteria overlap with those of psychoses: specifically, schizophrenia and bipolar disorder.
Until now, this list might have seemed impossibly confusing, but thanks to the diametric model of mental illness, hysteria begins to make sense and could even be seen to fulfill a controversial but implicit prediction of the model. According to the diametric model, psychotic spectrum disorders (PSDs) are the mentalistic opposite of autistic spectrum ones (ASDs). ASDs are hypo-mentalistic, meaning deficits in our innate ability to understand behavior in mental terms, but PSDs are hyper-mentalistic, with excessive mentalizing in all its forms.
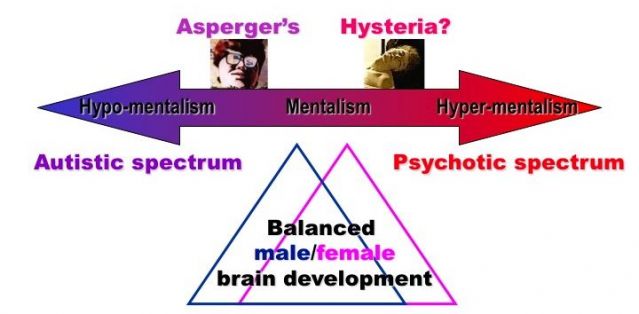
And this is the key to hysteria: according to the diametric model, hysteria looks like a high-functioning form of PSD, opposite to high-functioning ASD, notably Asperger’s syndrome (above). Once you see this, you can explain all the features:
- Historical and cultural contingency: to the extent it comprises social, cultural and inter-personal skills, mentalism is also historically and culturally contingent — and hyper-mentalism even more so.
- The female biased sex ratio: Asperger’s syndrome affects many more males than females, thanks to the fact the males are averagely somewhat less mentalistic than females, implying that high-functioning PSD should symmetrically affect more females.
- Suggestibility is a mentalistic trait epitomizing both empathy and other-directedness that sharply contrasts with the stubborn independence of mind and lack of empathy seen in ASD. Its limitations in curing hysteria suggest a less tractable underlying disorder.
- Element of Folie à deux/shared psychotic disorder: Shared attention is a key mentalistic skill, symptomatically deficient in ASD but hypertrophied in hypnosis and shared psychotic disorder.
- Deceit is a mentalistic skill strikingly — and very creditably — deficient in autism but hypertrophied in PSDs, notably in delusions.
- Parallels with religious manias: Religion epitomizes collective, cultural, and normalized hyper-mentalism, so the overlap with hysteria is predictable and easily understood.
- Thespian skills demand mentalistic gifts lacking in ASD but very common in PSD, as some recent experiments confirm.
- The literary dimension is inevitable, given that literary culture exploits mentalistic skills and imagery, particularly in the modern world, where fiction has been a major contributor to folk psychology.
- Overlap with PSD is obvious and predictable if hysteria is indeed a high-functioning form of psychosis.
But of course, that still leaves the question: Where have all the hysterics gone? One answer is that hysteria might have mutated into other manifestations of high-functioning PSD seen in today’s world, such as MPD, Borderline Personality Disorder, and perhaps eating disorders.
But another possibility suggested by the imprinted brain theory and diametric model is that whatever caused the epidemic of high-functioning PSD among women in the late 19th century Western world may have reversed and become a factor that is now causing its opposite: an epidemic of high-functioning ASD. I am already on record as suggesting rising living standards as the factor implicated in the latter, so conceivably its opposite could apply to hysteria and could be poor nutrition in urban areas associated with industrialization. Maternal starvation in pregnancy is a known risk factor for schizophrenia in resulting offspring, and in France surprisingly widespread wet-nursing by impoverished women may have been another similar but somewhat mitigated risk factor predisposing children to high-functioning, mild PSD as seen in hysteria.

